

Shoulder instability treatment in Abu Dhabi often starts with understanding why the shoulder repeatedly slips, dislocates, or feels unstable. Many patients describe the sensation as the shoulder “popping out” during sport or daily activities.
Have you ever felt your shoulder suddenly “pop out,” slip, or move in a way that felt unstable or unnatural?
For some patients, this happens during sports or after a fall. For others, the shoulder never fully dislocates but constantly feels loose, painful, or unreliable in certain positions. Many describe the sensation as if the shoulder is “about to come out” when reaching overhead, throwing, or rotating the arm backward.
This condition is known as shoulder instability, and it is one of the most common causes of recurrent shoulder problems in young and active individuals.
At Shoulder UAE, we frequently see patients with first-time dislocations, recurrent instability, labral injuries, and failed previous stabilization surgeries. Understanding the cause of instability is the first step toward choosing the right treatment.
What Is Shoulder Instability?
The shoulder is the most mobile joint in the human body. This remarkable range of motion allows us to lift, rotate, throw, push, and perform complex overhead activities.
However, this mobility comes at a cost: the shoulder is also one of the least inherently stable joints.
A simple way to understand shoulder anatomy is to imagine a golf ball sitting on a tee. The ball represents the humeral head (the top of the arm bone), while the tee represents the glenoid (the shoulder socket). Unlike the hip, where the ball sits deeply inside the socket, the shoulder socket is relatively shallow.
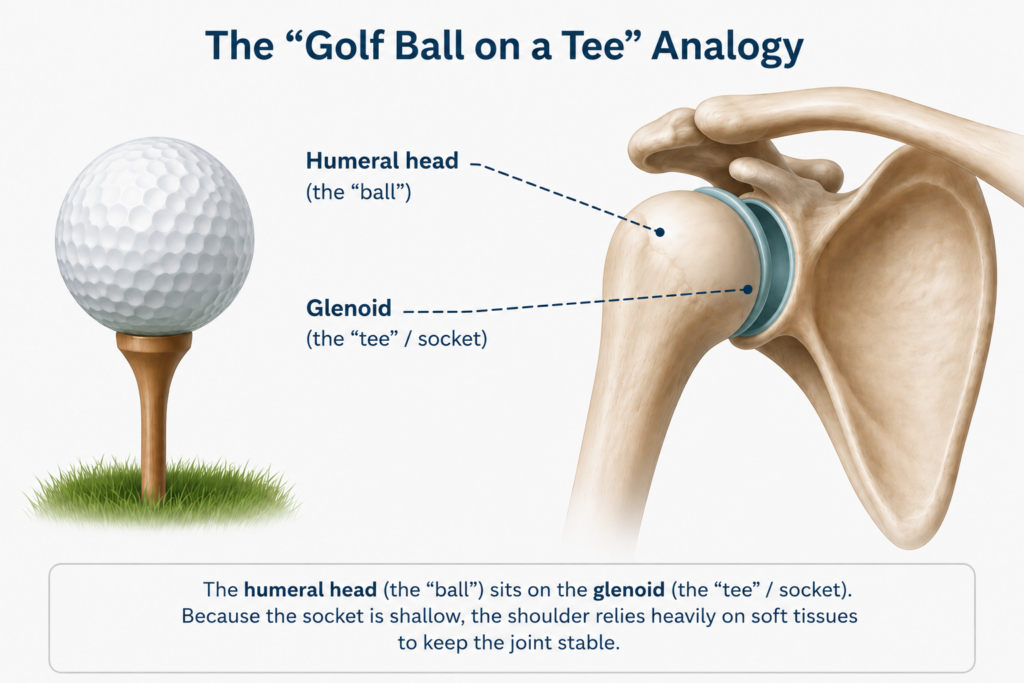
Because of this, shoulder stability depends heavily on soft tissue structures, including:
- The labrum (a ring of cartilage around the socket)
- The joint capsule
- The ligaments
- The rotator cuff muscles
- The muscles controlling the shoulder blade (scapula)
When one or more of these structures becomes damaged, stretched, or torn, the shoulder can become unstable.
What Is a Shoulder Dislocation?
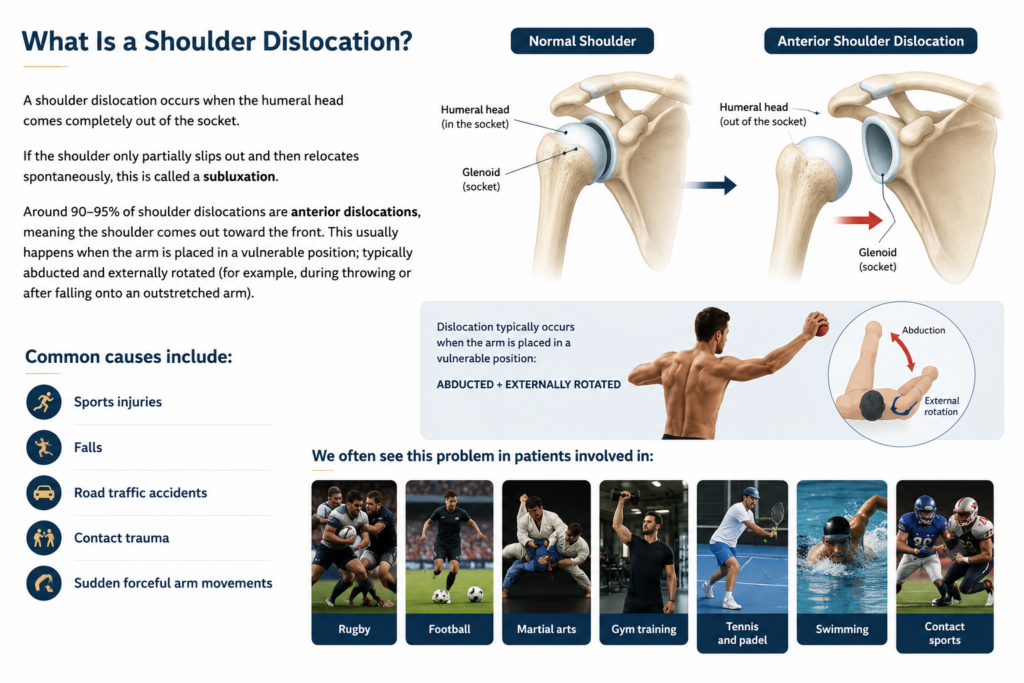
A shoulder dislocation occurs when the humeral head comes completely out of the socket.
If the shoulder only partially slips out and then relocates spontaneously, this is called a subluxation.
Around 90–95% of shoulder dislocations are anterior dislocations, meaning the shoulder comes out toward the front. This usually happens when the arm is placed in a vulnerable position; typically abducted and externally rotated (for example, during throwing or after falling onto an outstretched arm).
Common causes include:
- Sports injuries
- Falls
- Road traffic accidents
- Contact trauma
- Sudden forceful arm movements
We often see this problem in patients involved in:
- Rugby
- Football
- Martial arts
- Gym training
- Tennis and padel
- Swimming
- Contact sports
Why Does the Shoulder Become Unstable?
In many cases, the first dislocation causes structural damage inside the joint. Once these stabilizing structures are injured, the risk of future dislocations increases.
The exact cause varies from patient to patient.
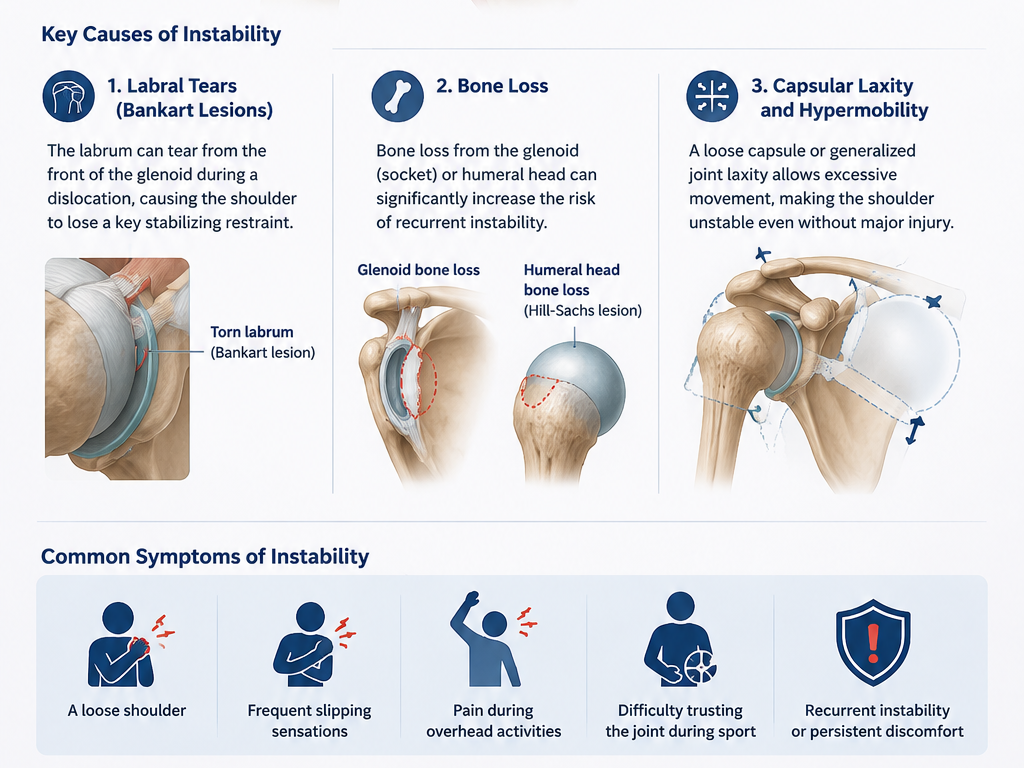
Labral Tears (Bankart Lesions)
One of the most common injuries associated with instability is a labral tear, particularly a Bankart lesion.
The labrum is a ring of fibrocartilage that surrounds the socket and helps deepen it, improving stability. It also serves as an attachment point for ligaments.
When the shoulder dislocates, the labrum can detach from the front of the glenoid. Once this happens, the shoulder loses one of its main stabilizing restraints.
Patients with labral tears often report recurrent slipping, painful clicking, or a persistent sensation of instability.
Bone Loss
Recurrent dislocations can progressively damage bone.
This may affect:
- The front edge of the glenoid (socket bone loss)
- The humeral head
One common injury is the Hill-Sachs lesion, a compression defect in the humeral head caused when the bone impacts against the socket during dislocation.
Why is this important? Because significant bone loss dramatically increases the chance of recurrent instability and may change the surgical strategy completely.
This is why proper imaging is essential before surgery.
Capsular Laxity and Hypermobility
Not all instability comes from trauma.
Some patients naturally have loose ligaments or generalized joint hypermobility. In these cases, the capsule and ligaments may be too elastic, allowing excessive movement of the humeral head.
These patients may experience instability even without a major injury.
They often describe symptoms such as:
- A loose shoulder
- Frequent slipping sensations
- Pain during overhead activities
- Difficulty trusting the joint during sport
Symptoms of Shoulder Instability
Symptoms can vary significantly depending on severity.
Some patients have had a dramatic dislocation requiring emergency reduction. Others experience subtle instability for years before diagnosis.
Common symptoms include:
- Shoulder dislocation or subluxation
- Recurrent slipping episodes
- Pain during overhead movement
- Clicking, clunking, or catching
- Weakness
- Loss of power in sport
- Apprehension in certain positions
- Fear of recurrence
One of the most characteristic symptoms is apprehension; the feeling that the shoulder may dislocate again when the arm is placed in a vulnerable position.
This often leads patients to avoid specific movements entirely.
Who Is at Higher Risk?
Not every patient who dislocates a shoulder will develop chronic instability.
However, recurrence is much more common in certain groups.
Higher-risk patients include:
- Young patients (especially under 25)
- Athletes
- Contact sports players
- Patients with hypermobility
- Patients with significant bone loss
- Individuals with previous instability surgery
Age matters greatly.
A first dislocation in a young athlete carries a very high recurrence risk. In some studies, recurrence rates in young active patients exceed 70–80% if treated non-operatively.
This is why management must be individualized.
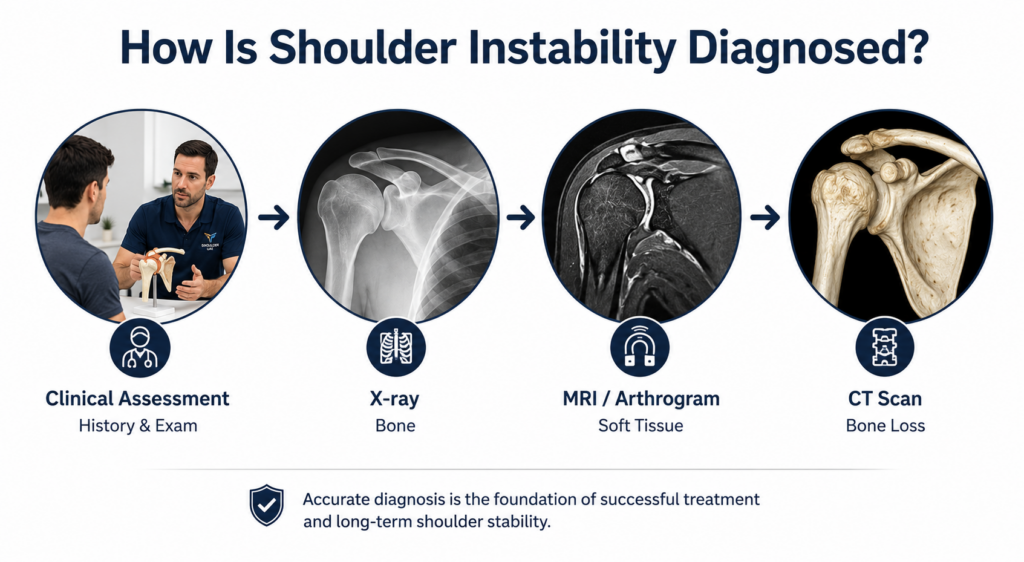
How Is Shoulder Instability Diagnosed?
Diagnosis starts with a detailed clinical assessment.
During consultation, I focus on several key questions:
- How did the injury happen?
- Was there a full dislocation?
- How many episodes have occurred?
- Does the shoulder feel unstable daily?
- Is there hypermobility?
- What sports or activities are important to the patient?
- Has there been previous surgery?
A physical examination then helps identify the direction and severity of instability.
Imaging is often required to understand the structural damage.
X-rays
X-rays are usually the first imaging step.
They help identify:
- Previous dislocation
- Fractures
- Bone defects
- Large Hill-Sachs lesions
- Glenoid bone loss
Although X-rays do not show soft tissues well, they remain extremely important.
MRI or MR Arthrogram
MRI is useful to assess soft tissue injuries.
This includes:
- Labral tears
- Ligament injuries
- Capsular damage
- Rotator cuff injuries
An MR arthrogram; where contrast is injected into the joint before the scan; can be particularly helpful for detecting subtle labral injuries that may be missed on a standard MRI.
This is especially valuable in younger athletic patients with suspected hidden instability lesions.
CT Scan
CT scanning provides the most accurate assessment of bone loss.
This becomes crucial in recurrent instability, revision surgery, or when planning procedures such as a bone block or Latarjet.
In complex cases, CT can completely change the treatment plan.
Can Shoulder Instability Be Treated Without Surgery?
Yes; some patients can improve without surgery.
Conservative treatment typically includes physiotherapy focused on improving dynamic stability around the shoulder.

This may involve:
- Rotator cuff strengthening
- Scapular stabilization
- Postural correction
- Proprioception training
- Activity modification
The goal is to improve muscular control and compensate for structural instability.
Non-surgical treatment is often more suitable for:
- Older patients
- Lower-demand individuals
- First-time dislocations
- Patients with minimal structural damage
However, physiotherapy cannot repair a detached labrum or restore lost bone.
That distinction is important.
When Is Surgery Recommended?
Surgery is often recommended when instability becomes recurrent or significantly affects function.
Common indications include:
- Recurrent dislocations
- Repeated subluxations
- Structural labral tears
- Significant bone loss
- Failed rehabilitation
- High-demand athletic profile
- Previous failed surgery
The goal of surgery is straightforward:
Restore stability while preserving motion and function.
Choosing the right operation depends entirely on the cause of instability.
Surgical Treatment Options
Arthroscopic Bankart Repair
This is one of the most common procedures for traumatic anterior instability.
Using minimally invasive arthroscopic surgery, the detached labrum is repaired back to bone using suture anchors.
This restores tension to the capsule and ligaments and helps re-establish stability.
It works particularly well in patients with minimal bone loss.

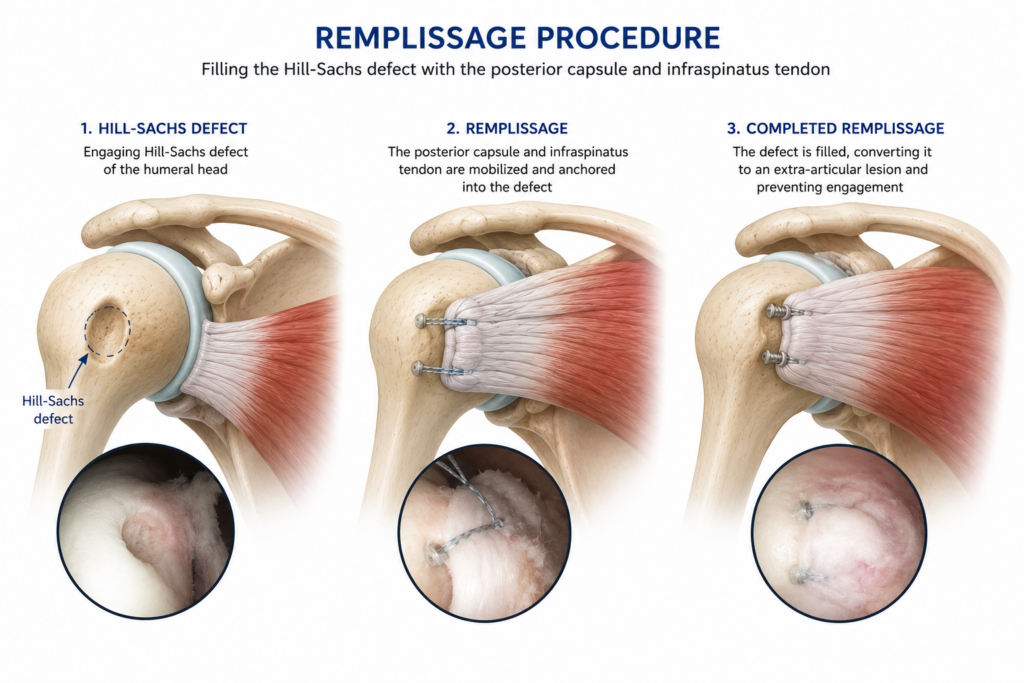
Remplissage
Some patients have an engaging Hill-Sachs lesion contributing to recurrent instability.
In these cases, a procedure called remplissage may be added to a Bankart repair.
This reduces engagement of the defect and improves stability.
Bone Block Procedures / Latarjet
When significant bone loss exists, soft tissue repair alone may not be enough.
In these cases, a bone augmentation procedure such as a Latarjet may be recommended.
This restores the anterior socket and provides additional dynamic stability.

Bone block procedures are often used in:
- Recurrent instability
- Contact athletes
- Failed previous surgery
- Significant glenoid bone loss
Recovery After Surgery
Recovery depends on the type of surgery performed.

Typical recovery follows this timeline:
First 4–6 Weeks
The arm is protected in a sling while healing begins. Early rehabilitation focuses on safe movement and protecting the repair.
6–12 Weeks
Range of motion improves gradually, and strengthening begins.
3–6 Months
Sports-specific rehabilitation progresses.
Return to contact sports or high-demand activities usually requires careful assessment.
Full recovery may take 4 to 8 months, depending on the procedure and the demands of the patient.
When Should You See a Shoulder Specialist?
You should seek specialist assessment if:
- Your shoulder has dislocated
- It repeatedly slips or feels unstable
- You avoid movements due to fear
- You have persistent pain after a dislocation
- Your performance in sport is declining
- You had previous surgery but still feel unstable
Early diagnosis matters.
Every recurrent dislocation can cause additional damage to cartilage, labrum, or bone.
International guidelines from organizations such as the ASES support specialist assessment after recurrent dislocation.
Final Thoughts
Shoulder instability can be frustrating, painful, and psychologically limiting. Many patients lose confidence in their shoulder long before they lose actual strength.
The key to successful treatment is understanding why the shoulder is unstable.
Is the problem due to:
- A labral tear?
- Bone loss?
- Capsular laxity?
- A failed previous surgery?
Once the true cause is identified, treatment can be tailored accordingly.
At Shoulder UAE, I provide specialist assessment and advanced treatment for:
- First-time shoulder dislocations
- Recurrent instability
- Labral tears
- Failed Bankart repairs
- Failed Latarjet procedures
- Complex revision instability surgery
The goal is always the same:
Restore stability, confidence, and function so you can safely return to daily life, work, and sport.
Frequently Asked Questions
Some patients improve with physiotherapy, especially after a first-time dislocation. However, recurrent instability often requires surgery.
Young active patients have a higher recurrence risk after a first dislocation.
Bankart repair restores the labrum, while Latarjet restores bone loss using the coracoid.
You should seek specialist assessment after any dislocation or recurrent instability episode.